It’s natural for parents of children recently diagnosed to ask what caused the development of their child’s scoliosis, and while idiopathic scoliosis has no known cause, there does appear to be a genetic link. Regardless of the cause, scoliosis should be treated proactively.
While there has yet to be a specific gene identified that explains the onset of idiopathic scoliosis, there do appear to be genetic factors; having a family history is considered a risk factor, but this could also be on account of familial and/or other shared factors.
Scoliosis has been around for hundreds of years, but in most cases, we still don’t fully understand what causes its initial onset, but we do know how to treat it effectively.
What Causes Scoliosis?
It’s estimated that there are close to seven million people living with scoliosis in the United States alone, so education and awareness is important.
Scoliosis is a structural spinal condition that causes an unnatural lateral spinal curve that rotates to develop, and while it affects all ages, it’s most commonly diagnosed in children (5).
Adolescent idiopathic scoliosis is the most prevalent type of scoliosis overall, and as a progressive condition, the nature of scoliosis is to become more severe over time and with growth (2).
There are also different types of scoliosis with different causes, and while most conditions are idiopathic, approximately 20 percent of cases have known causes.
Known Causes of Scoliosis
Neuromuscular scoliosis can develop as a secondary complication of a serious neuromuscular disorder such as spina bifida, muscular dystrophy, or cerebral palsy; neuromuscular conditions can interrupt communication between the brain, the spine, the muscles and connective tissues that support the spine.
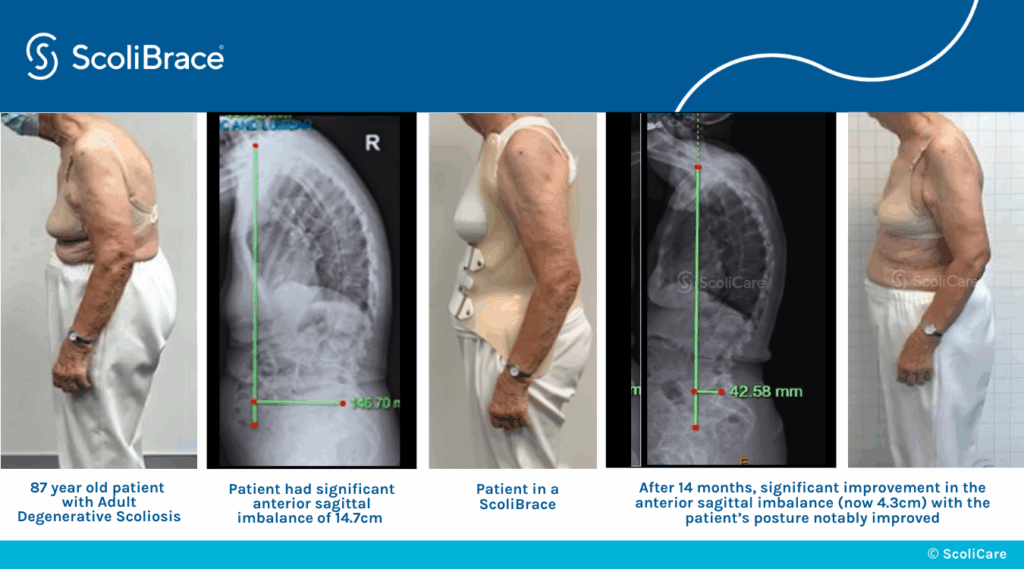
Degenerative scoliosis is caused by degenerative changes in the spine, commonly involving the intervertebral discs, so it affects older adults and can put them at risk of injury through a fall.
Cases of congenital scoliosis are rare and affect babies born with scoliosis due to a spine that didn’t form properly in utero.
The vast majority of known scoliosis cases, however, involve idiopathic scoliosis, and a lot of time and effort has gone into studying the potential causes of idiopathic scoliosis (1).
Idiopathic Scoliosis
Idiopathic means no known cause, or more specifically, no single-known cause. When it comes to idiopathic scoliosis, it’s been suggested that causation is multifactorial: involves a number of factors.
The most common age to be diagnosed with scoliosis is between 10 and 18 years, and adolescents are also the most at risk for rapid progression due to the unpredictable nature of pubescent growth spurts (2).
To parents of adolescents, scoliosis can appear to develop overnight, but as the early signs of scoliosis can be subtle, it’s more likely that the scoliosis had developed earlier and a recent growth spurt triggered progression that made its effects more noticeable.
As a condition that’s always changing, when scoliosis is diagnosed doesn’t necessarily indicate it has recently developed, but more so that its effects have recently become noticeable enough to alert parents to the need for assessment (2, 7).
Parents of adolescents recently diagnosed commonly ask if scoliosis is hereditary, and this doesn’t have a clear answer.
Is Idiopathic Scoliosis Hereditary?
As the leading cause of unnatural spinal curves in school-aged children, scoliosis prevalence is taken seriously, and many studies have attempted to identify a gene, or genetic mutation, that accounts for the onset of idiopathic scoliosis (1).
Although a scoliosis gene has yet to be identified, having scoliosis in the family is considered a common risk factor, but remember, families don’t just share genes, they share many common factors: environmental, societal, financial, diet, lifestyle, body type, posture and more.
It’s been suggested that these factors, or a combination of these factors, could contribute to the onset of idiopathic scoliosis.
It’s important to note, however, that there are many cases of idiopathic scoliosis diagnosed in families with no prior history, but this can also be difficult to clearly determine as scoliosis isn’t always easy to diagnose and many people live with scoliosis unaware.
Early Detection and Intervention
There are no treatment guarantees, but early diagnosis is key to treatment success, so knowledge of what risk factors mean and the early signs of scoliosis have a number of benefits (7).
Having a risk factor means screening should be performed because developing scoliosis is more likely.
In most cases of childhood scoliosis, the appearance of abnormal posture is the earliest sign of scoliosis: uneven shoulders, shoulder blades, and uneven hips, and in adults, it’s most often pain that leads to an assessment and diagnosis (5).
What Mild Scoliosis Really Means
Early detection is directly linked to treatment success because it can mean starting treatment while conditions are still mild; while the term mild can suggest a lack of urgency, this is the best time to act (7).
It’s important for parents to understand that just because a condition is mild at the time of diagnosis doesn’t mean there is more time to decide on a course of treatment, or that treatment is less urgent (2, 5, 7).
There are a lot of factors that go into determining scoliosis severity; while curve size is the main guideline, the curve’s flexibility and rate of progression are additional factors that need to be considered.
Mild curves are smaller and simpler to correct, so with progressive conditions like scoliosis, the sooner treatment is started, the better.
As scoliosis progresses, it’s becoming more severe, the size and rotation of the unnatural spinal curve is increasing, condition effects are becoming more noticeable, and the condition is becoming more complex to treat.
So what a diagnosis of mild scoliosis really means is that the potential benefit of early intervention is available, but only to those who commit to a proactive treatment plan that’s started immediately following a diagnosis (7).
And if a child diagnosed with mild scoliosis has siblings, the siblings should be screened and watched closely for the development of abnormal posture.
The benefit of being aware of a family history, and what it means, is that it can alert parents to the need for early screening and can lead to early detection and intervention.
Scoliosis Screening
Scoliosis screening is a process of checking for indicators of scoliosis, particularly in young patients who are more likely to be diagnosed, such as those with a family history (7).
There are a number of benefits associated with early detection and starting treatment prior to the first pubescent growth spurt; remember, progression is triggered by growth.

In addition to a family history, gender and age are additional risk factors; adolescent females are the most likely to be diagnosed, and screening can be started at a young age as part of regular check ups.
During periods of rapid growth, children should be assessed more regularly.
Forward Bend Assessment
Scoliosis screening commonly involves a standing assessment and what’s known as an adam’s forward bend test that can help identify children with scoliosis (7).
The spine is most visible when in a forward bend position, so during an adams forward bend test, a patient will bend forward at the hips as if trying to touch their toes, and in this position, the spine and trunk are examined for asymmetries.
In some cases, the spine’s unnatural curve can be visible, as are related trunk asymmetries like uneven shoulders, shoulder blades, hips, and a rib cage asymmetry.
Particularly if there is a family history of scoliosis, children can benefit from regular screening to facilitate early diagnosis.
If a screening examination finds indicators of scoliosis, further testing may be warranted in the form of a scoliosis X-ray.
Conservative treatment options are less limited the sooner they are applied, and the longer the postural changes caused by scoliosis are in place, the harder they can be to improve/reverse.
As scoliosis progresses, the spine gets more rigid, and this can make it less responsive to treatment; this is why early detection is key because it means treatment can be started while conditions are still mild and more likely to be responsive.
Severe curves are harder to correct, and the goal of proactive treatment is to prevent mild scoliosis from becoming moderate and severe scoliosis.
Conclusion
Although genetic factors are thought to play a role in idiopathic scoliosis causation, scoliosis isn’t classified as hereditary.
Idiopathic scoliosis is considered to be multifactorial, with familial factors to consider.
Scoliosis in children needs to be taken seriously; as a progressive condition triggered by growth, early diagnosis is key.
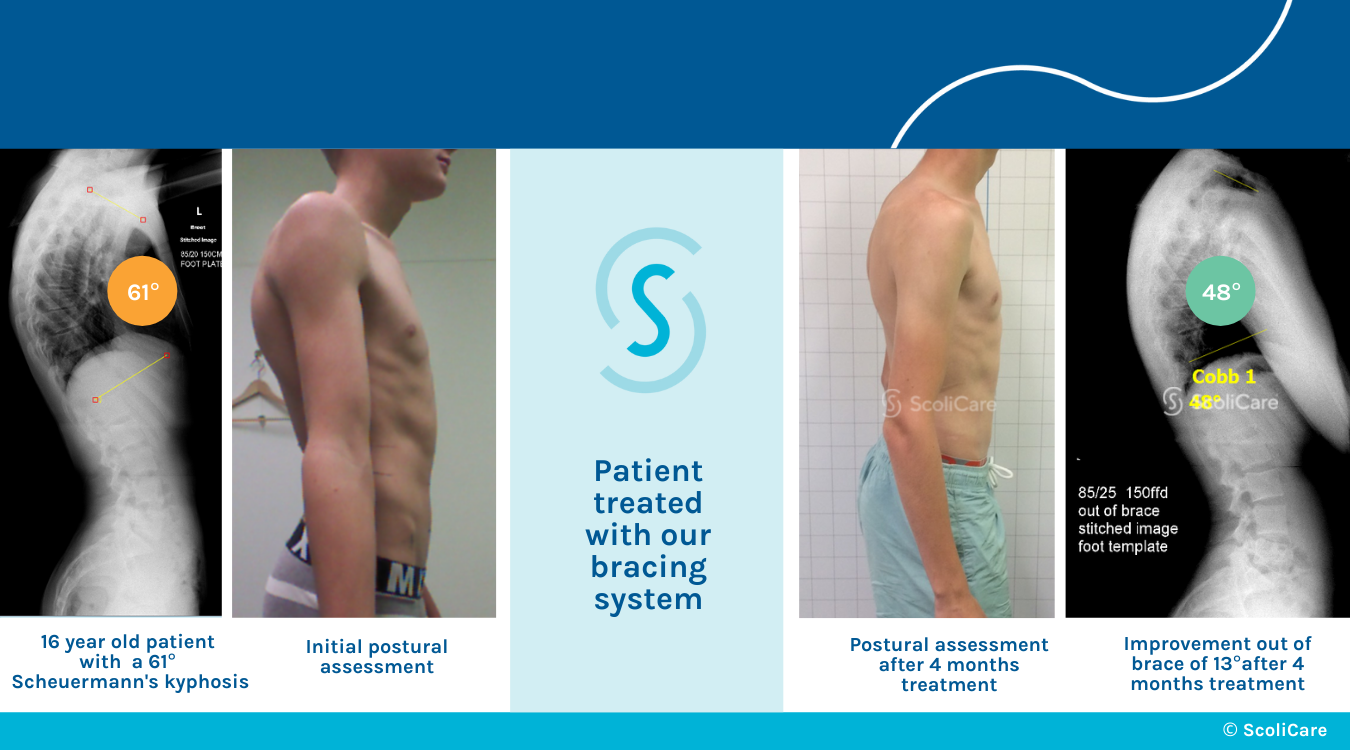
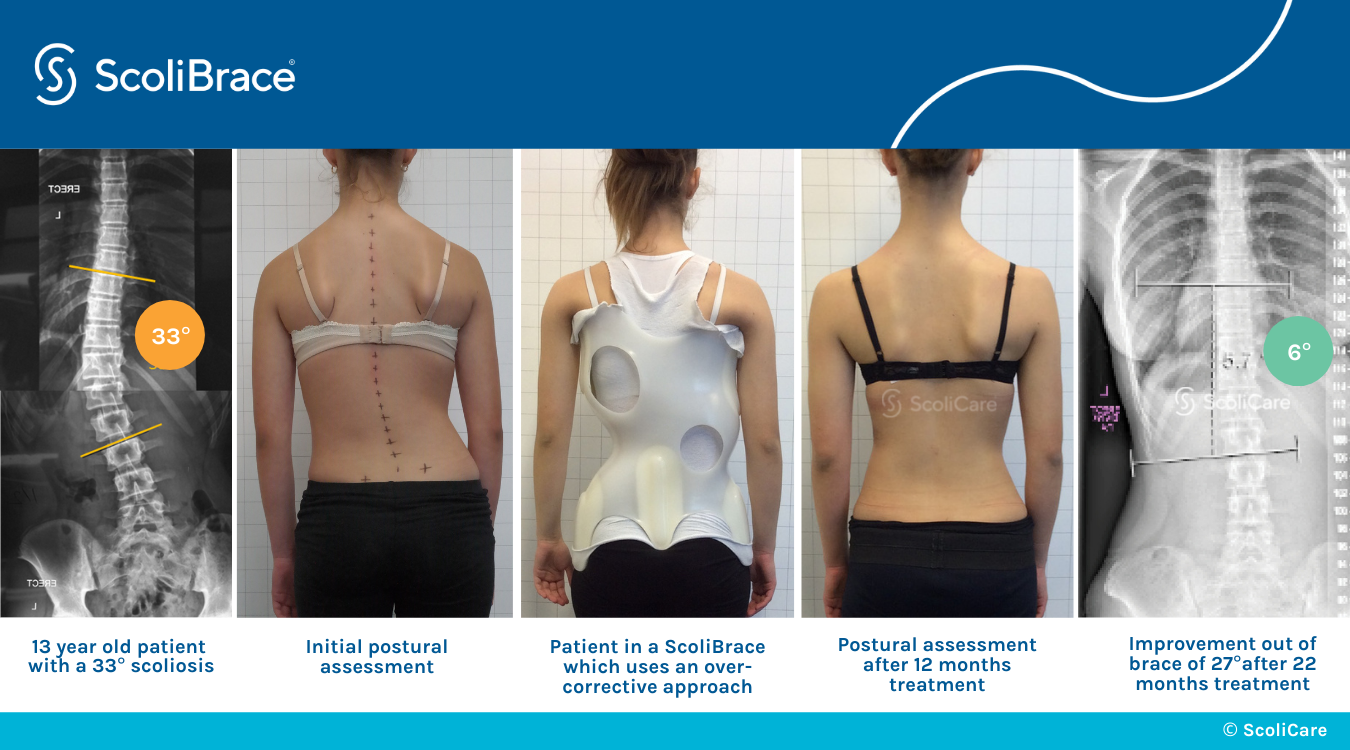
What’s most important about a scoliosis diagnosis is how it’s responded to with treatment. Mild scoliosis can be highly responsive, and here at ScoliCare, customized treatment involves the integration of effective conservative treatment options: ScoliBrace® and ScoliBalance®.
Regardless of what causes scoliosis to develop initially, what becomes more important is how the condition is managed. Scoliosis can be highly treatable, particularly with early detection.
When corrective bracing and scoliosis-specific exercise are combined, the spine’s surrounding muscle balance and strength may be improved, along with the spine’s balance, stability, and flexibility; as the health of the spine and its surroundings are improved, the effects can be felt throughout the body.
So whether or not a child’s scoliosis develops because of genetic, environmental, or familial factors, the best time to start treatment and work towards improvement is always now.
We have clinicians that are uniquely qualified to prescribe the Scolibrace. In addition to these, we are one of only a few clinics in Canada that are able to prescribe scoliosis specific exercises using the SEAS and Scolibalance methods. When used in conjunction, these various treatment methods can significantly improve the quality of our patient’s lives and help reduce the impact of Scoliosis and Hyperkyphosis on the body.
References:
- A Grauers, E Einarsdottir P Gerdhem. Genetics and Pathogenesis of Idiopathic Scoliosis: National Library of Medicine
- Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis: National Library of Medicine
- Weinstein SL. The Natural History of Adolescent Idiopathic Scoliosis. J Pediatr Orthop. 2019 Jul;39(Issue 6, Supplement 1 Suppl 1):S44-S46. doi: 10.1097/BPO.0000000000001350. PMID: 31169647.
- Marchese R, Du Plessis J, Pooke T, McAviney J. The Improvement of Trunk Muscle Endurance in Adolescents with Idiopathic Scoliosis Treated with ScoliBrace® and the ScoliBalance® Exercise Approach. J Clin Med. 2024 Jan 23;13(3):653. doi: 10.3390/jcm13030653. PMID: 38337346; PMCID: PMC10856658.
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, Lebel A, Marti C, Maruyama T, O’Brien J, Price N, Parent E, Rigo M, Romano M, Stikeleather L, Wynne J, Zaina F. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018 Jan 10;13:3. doi: 10.1186/s13013-017-0145-8. PMID: 29435499; PMCID: PMC5795289.
- Scoliosis in Children and Teens: National Institute of Arthritis and Musculoskeletal and Skin Diseases
- Comparison of Functional Outcome and Quality of Life in Patients With Idiopathic Scoliosis Treated by Spinal Fusion: National Library of Medicine
- Screening for the Early Detection of Idiopathic Scoliosis in Adolescents: American Academy of Orthopaedic Surgeons
- Marty-Poumarat, Catherine MD*; Scattin, Luciana MD†; Marpeau, Michèle MD*; Garreau de Loubresse, Christian MD‡; Aegerter, Philippe MD, PhD§. Natural History of Progressive Adult Scoliosis. Spine 32(11):p 1227-1234, May 15, 2007. | DOI: 10.1097/01.brs.0000263328.89135.a6